Human curiosity has always been driven by a desire to understand the universe in simple, logical terms. Yet, sometimes nature answers our questions with a riddle, a contradiction, or what scientists call a paradox. Paradoxes are situations that defy intuition or challenge the way we think reality should behave. They can be thought of as intellectual knots—puzzles that seem to say, “Wait… how can that be true?”
When we step into the world of quantum mechanics—the branch of physics that studies the smallest particles in existence—paradoxes don’t just appear occasionally; they seem to be everywhere. The deeper we look, the more we realize that the universe doesn’t always play by the rules we thought we knew.
What Is a Paradox?
A paradox occurs when two apparently contradictory ideas or facts both seem true at the same time. Some paradoxes are just misunderstandings of language or logic. Others, especially in science, are genuine phenomena where reality behaves in ways that challenge our understanding.
For example:
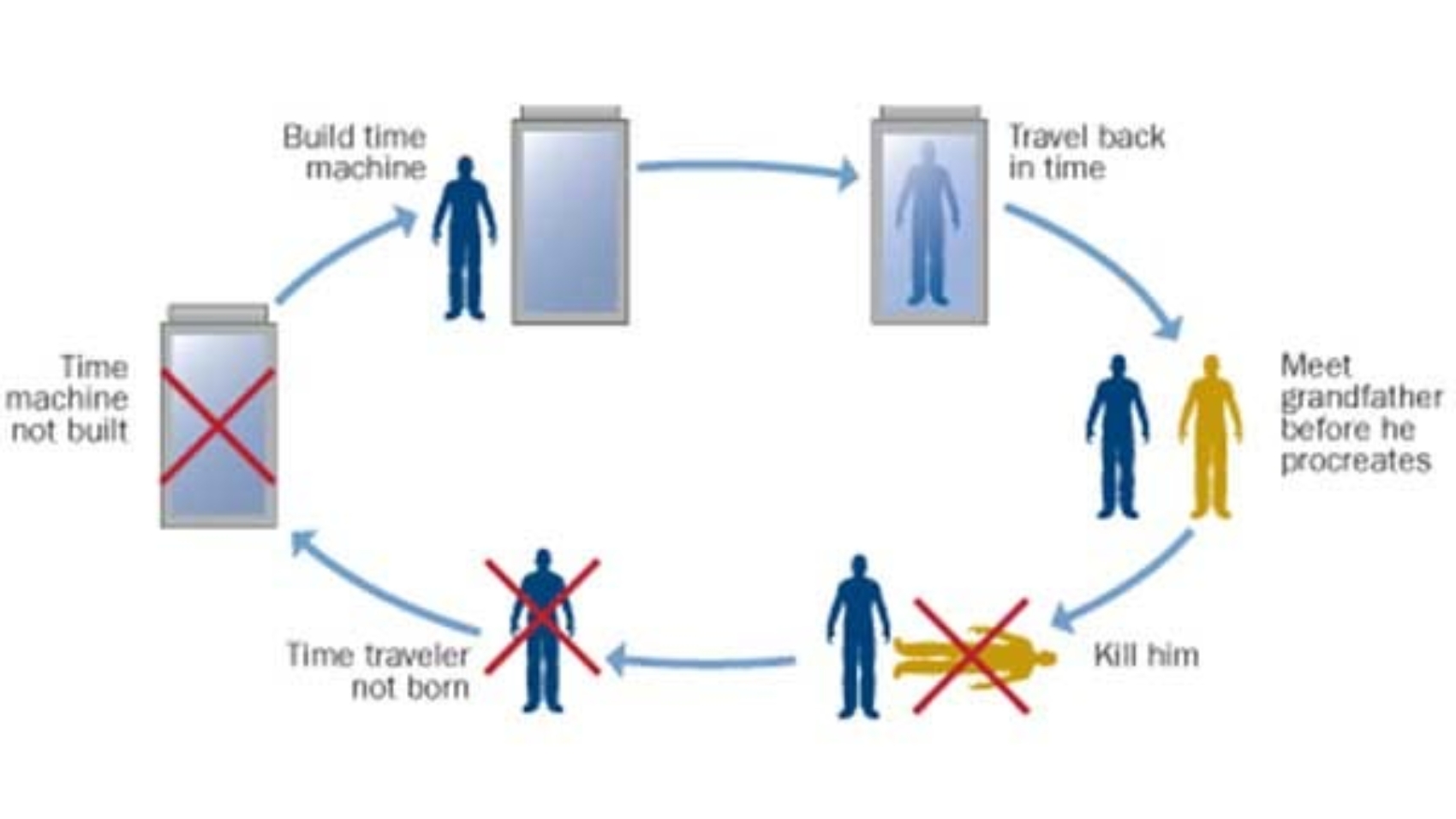
- In the grandfather paradox, if you travel back in time and prevent your grandfather from meeting your grandmother, you wouldn’t be born—but if you were never born, how could you travel back to stop them from meeting?
- In the liar paradox, the statement “This sentence is false” can’t be consistently labeled as true or false.
While these are thought experiments, quantum mechanics introduces real-life situations where paradox-like behavior is measurable and repeatable.
Quantum Mechanics: The Playground of Paradox
Quantum mechanics deals with the behavior of particles like electrons, photons, and atoms. These particles exist at scales so small that the classical laws of physics—like Newton’s laws—stop working in a predictable way.
Instead, particles in the quantum realm seem to obey strange rules:
- They can exist in multiple states at the same time (superposition).
- They can be linked across space instantly (entanglement).
- They don’t seem to have definite properties until measured (wavefunction collapse).
These behaviors often sound like science fiction, but they’ve been confirmed repeatedly by experiments. The challenge is that they don’t match how we experience the everyday world, which is why so many paradoxes arise.
Famous Quantum Paradoxes
- Schrödinger’s Cat
Proposed by physicist Erwin Schrödinger in 1935, this thought experiment involves a cat in a sealed box with a quantum trigger that has a 50% chance of killing it. Quantum theory says that until we open the box and observe the cat, it’s both alive and dead—a superposition of states. This is not a literal suggestion about cats, but a way to highlight the weirdness of applying quantum rules to larger objects.
2. The EPR Paradox
In 1935, Einstein, Podolsky, and Rosen proposed a paradox to challenge quantum mechanics. They argued that if two particles are entangled and separated by vast distances, a measurement on one instantly affects the other—implying “spooky action at a distance.” Einstein thought this meant quantum theory was incomplete. Later experiments confirmed that entanglement is real and instantaneous, even if it defies classical logic.
3. The Quantum Zeno Effect
This paradox says that a quantum system’s evolution can be “frozen” by constantly observing it. In other words, the act of measurement can stop change from happening—something that sounds impossible but has been observed experimentally.
Why Do Quantum Paradoxes Matter?
These paradoxes are more than brain teasers. They are clues that our everyday assumptions about reality may be incomplete. In fact, quantum mechanics has given rise to revolutionary technologies:
- Quantum computers that can solve problems classical computers can’t.
- Quantum cryptography for ultra-secure communication.
- Quantum sensors with precision far beyond current limits.
By wrestling with paradoxes, scientists often discover deeper truths about the universe.
Philosophical Implications
Quantum paradoxes force us to ask fundamental questions:
- Is reality objective, or does it depend on observation?
- Do particles exist in a definite state before we look?
- Is the universe deterministic, or does chance play a fundamental role?
These questions blur the line between physics and philosophy, showing that understanding the universe isn’t just about equations—it’s about rethinking what “reality” means.
Conclusion
Paradoxes in quantum mechanics remind us that nature is under no obligation to conform to human intuition. The universe operates according to its own principles, even if they seem contradictory or strange to us. By exploring these paradoxes, scientists aren’t just solving puzzles—they’re peeling back layers of reality itself.
Quantum mechanics may be full of mystery, but it’s through grappling with these mysteries that we expand the boundaries of human knowledge. And perhaps, in the process, we’ll come to see that the universe’s most puzzling paradox is not how strange it is—but how perfectly it works.