Chimeric Antigen Receptor T-cell (CAR-T) therapy has marked a groundbreaking advancement in the fight against cancer, bringing renewed optimism to patients facing previously untreatable forms of the disease. This innovative treatment harnesses the power of the immune system by genetically modifying a patient’s own T cells to target and destroy cancer cells with exceptional precision. Since its clinical debut in the early 2010s, CAR-T therapy has transformed the landscape of oncology, particularly for hematological malignancies, and continues to expand its potential for broader applications. This overview explores the underlying science, clinical uses, challenges, and the promising future of CAR-T cell therapy, highlighting its pivotal role in the evolving field of medicine as of 2025.
What is CAR-T Cell Therapy?
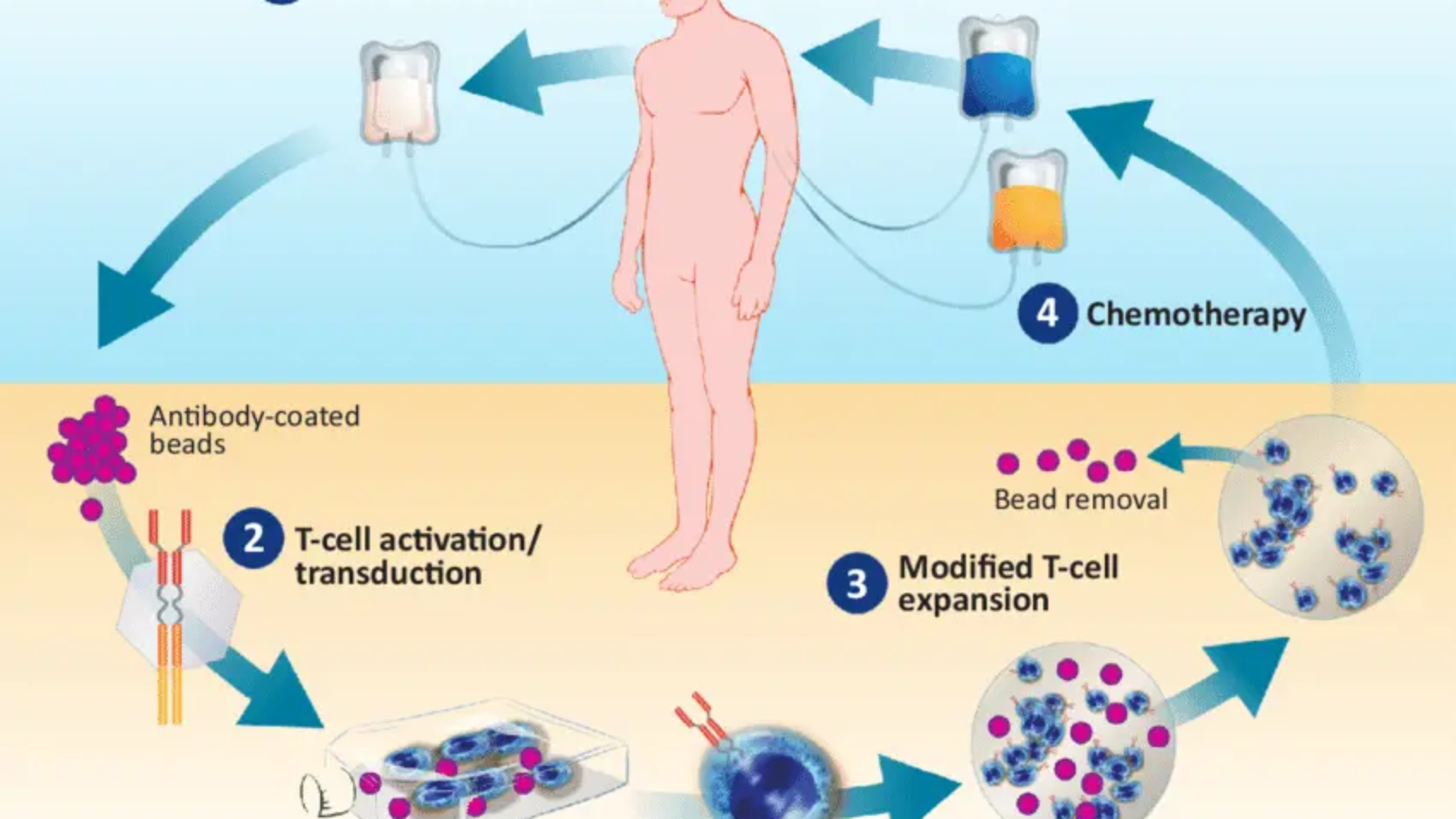
CAR-T cell therapy represents a form of immunotherapy that modifies a patient’s own T cells—key players in the immune system—to identify and eliminate cancer cells. This transformative treatment involves several critical steps:
- T-Cell Collection: The patient’s T cells are extracted from the bloodstream using a technique called leukapheresis.
- Genetic Modification: In the laboratory, these T cells are genetically engineered to express chimeric antigen receptors (CARs)—artificial proteins designed to recognize specific antigens present on cancer cells.
- Expansion: The engineered T cells are then multiplied in the lab, producing hundreds of millions of CAR-T cells.
- Infusion: These bioengineered T cells are infused back into the patient, where they seek out and destroy cancer cells that carry the target antigen.
- Monitoring: Following the infusion, patients are closely monitored for treatment response and potential side effects. Since CAR-T cells can persist in the body, they provide ongoing immune surveillance against the cancer.
CARs typically consist of an extracellular domain that binds to a cancer-specific antigen (such as CD19 in B-cell cancers), a transmembrane domain, and intracellular signaling domains that activate the T cell upon contact with the antigen. This design enables CAR-T cells to function like precision-guided missiles, homing in on cancer cells while sparing healthy tissue.
Current Applications
As of 2025, CAR-T cell therapy is primarily utilized for the treatment of blood cancers, with six FDA-approved therapies available:
- Tisagenlecleucel (Kymriah): Approved for B-cell acute lymphoblastic leukemia (ALL) and certain types of non-Hodgkin lymphomas (NHL).
- Axicabtagene ciloleucel (Yescarta): Approved for diffuse large B-cell lymphoma (DLBCL) and follicular lymphoma.
- Brexucabtagene autoleucel (Tecartus): Approved for mantle cell lymphoma and adult ALL.
- Lisocabtagene maraleucel (Breyanzi): Approved for DLBCL and other B-cell lymphomas.
- Idecabtagene vicleucel (Abecma): Targets multiple myeloma by focusing on the B-cell maturation antigen (BCMA).
- Ciltacabtagene autoleucel (Carvykti): Also approved for multiple myeloma.
These therapies have demonstrated remarkable success, achieving complete remission rates of 80–90% in some patients with relapsed or refractory B-cell ALL and sustained responses in 40–60% of DLBCL patients. CAR-T therapy has been especially transformative for patients who have exhausted other treatments, such as chemotherapy and stem cell transplantation.
Challenges and Side Effects
Even with its potential, however, CAR-T therapy is fraught with challenges:
1.Toxicity: CAR-T therapy can lead to significant side effects, including:
- Cytokine Release Syndrome (CRS): A dangerous surge of cytokines released by expanding T cells, often causing fever, low blood pressure, and organ dysfunction.
- Neurotoxicity: Immune effector cell-associated neurotoxicity syndrome (ICANS) can result in confusion, seizures, or brain swelling.
- Off-Target, Off-Tumor Effects: CAR-T cells may attack normal cells that express low levels of the target antigen, leading to unintended toxicity.
2. High Cost: Treatment is extremely expensive, ranging from $373,000 to $475,000 per course, not including hospitalization or follow-up care. This financial burden limits accessibility, particularly in resource-limited settings.
3. Manufacturing Complexity: Producing individualized CAR-T cells is time-consuming (taking 2–4 weeks) and requires specialized, high-tech facilities, which presents logistical challenges.
4. Limited Scope: Current CAR-T therapies are mainly effective against blood cancers. Solid tumors, which make up the majority of cancers, are harder to target due to diverse antigens, immunosuppressive tumor environments, and physical barriers.
5. Relapse: Some patients experience relapse because cancer cells lose the targeted antigen (e.g., no longer express CD19) or because CAR-T cells become exhausted.
Advances and Innovations in 2025
New studies are overcoming these challenges, expanding the scope of CAR-T therapy:
- Next-Generation CARs: Advanced CAR designs incorporate multiple signaling domains or target two antigens simultaneously to improve effectiveness and prevent relapse. For example, bispecific CARs are engineered to recognize both CD19 and CD22 antigens at the same time, reducing the risk of antigen escape.
- Solid Tumor Research: Researchers are working to adapt CAR-T therapy for use against solid tumors such as glioblastoma and pancreatic cancer. Efforts include targeting antigens like HER2 or EGFRvIII and combining CAR-T therapy with checkpoint inhibitors to overcome the immunosuppressive tumor microenvironment and enhance treatment effectiveness.
- Off-the-Shelf CAR-T: Allogeneic CAR-T therapies, derived from healthy donors or induced pluripotent stem cells (iPSCs), aim to reduce manufacturing time and costs, thereby increasing patient access. Companies like Allogeneic Therapeutics are leading clinical trials exploring this promising approach.
- Improved Safety: Strategies to minimize toxicity include “suicide switches” or “off switches” (such as iCasp9), which can deactivate CAR-T cells if severe side effects occur. Additionally, enhanced CAR designs are being developed to reduce the risks of cytokine release syndrome (CRS) and neurotoxicity.
- Combination Therapies: CAR-T therapy is increasingly being combined with other treatments, such as PD-1 inhibitors or chemotherapy, to boost effectiveness—particularly in tackling solid tumors.
- Beyond Cancer: Emerging research is exploring the use of CAR-T therapy for conditions beyond cancer, including autoimmune diseases like lupus, where CAR-T cells target harmful B cells, as well as infectious diseases such as HIV.
Future Potential
- Broader Indications: Successful application in solid tumors may establish CAR-T therapy as a frontline cancer treatment, potentially replacing many conventional therapies.
- Personalized and Accessible: Integration with AI and bioinformatics could streamline CAR-T design, enabling personalized therapies tailored to each patient’s tumor profile while lowering costs.
- Global Reach: Improvements in manufacturing and cost reduction strategies may make CAR-T therapies affordable and accessible in low- and middle-income countries, helping to bridge global healthcare disparities.
Conclusion
CAR-T cell therapy represents a paradigm shift in cancer treatment, offering unprecedented hope for patients with relapsed or refractory blood cancers. Its ability to reprogram the immune system to precisely target cancer cells showcases the remarkable power of biotechnology. While challenges such as toxicity, high costs, and limited effectiveness against solid tumors remain, research in 2025 is rapidly overcoming these hurdles. From allogeneic CAR-T therapies and dual-targeting CARs to expanding applications beyond cancer, CAR-T therapy stands poised to revolutionize medicine, turning personalized, curative treatments into a reality for millions.
For more information on the latest CAR-T innovations, explore resources at clinicaltrials.gov or follow updates from leading biotech companies like Novartis, Gilead Sciences, and Bristol Myers Squibb.

Author Name
Aradhy Shrivastav
Gr8 going Aradhay! keep writting…well done.